Extending primary care at scale: Early APCM outcomes from AMGA 2026

At this year’s AMGA Annual Conference, Cadence and Lifepoint Health shared early results from its preventive primary care program (APCM) designed to extend care beyond the traditional visit.
The poster, presented by Cadence CMO Dr. Eve Cunningham and Lifepoint CMO Dr. Chris Frost evaluated improvement in quality metrics, including preventive care gap closure, social needs coordination, and expansion of primary care capacity.
Why APCM Exists
Across health systems, primary care teams are being asked to manage increasingly complex Medicare populations, often without the infrastructure to do so between visits.
Patients with multiple chronic conditions require more than a few appointments per year. Care gaps accumulate, social needs go unaddressed, and follow-up is inconsistent.
APCM is designed to extend primary care between visits combining AI-enabled care plans with a dedicated clinical team to identify and close care gaps and support patients longitudinally. In practice, the program supports patients between visits through outreach and coordination – from scheduling appointments and managing refills to following up on preventive care and helping address needs like transportation, food, and housing.
Importantly, this work is aligned to each health system’s existing quality framework, not layered alongside it.
A complex population
The Lifepoint APCM cohort reflects the reality many health systems face:
- 99.8% of patients have two or more chronic conditions
- High prevalence of hypertension (83%), hyperlipidemia (84%), and diabetes (38%)
- Additional burden from COPD, obesity, and musculoskeletal disease
Despite this complexity, engagement remained strong:
- 92% active at three months
- 82% at six months
This level of sustained engagement is critical to driving longitudinal outcomes.
Early movement in preventive care
Within a 120-day period, APCM drove measurable improvement across multiple preventive care metrics all tracked directly against Lifepoint’s existing scorecard.
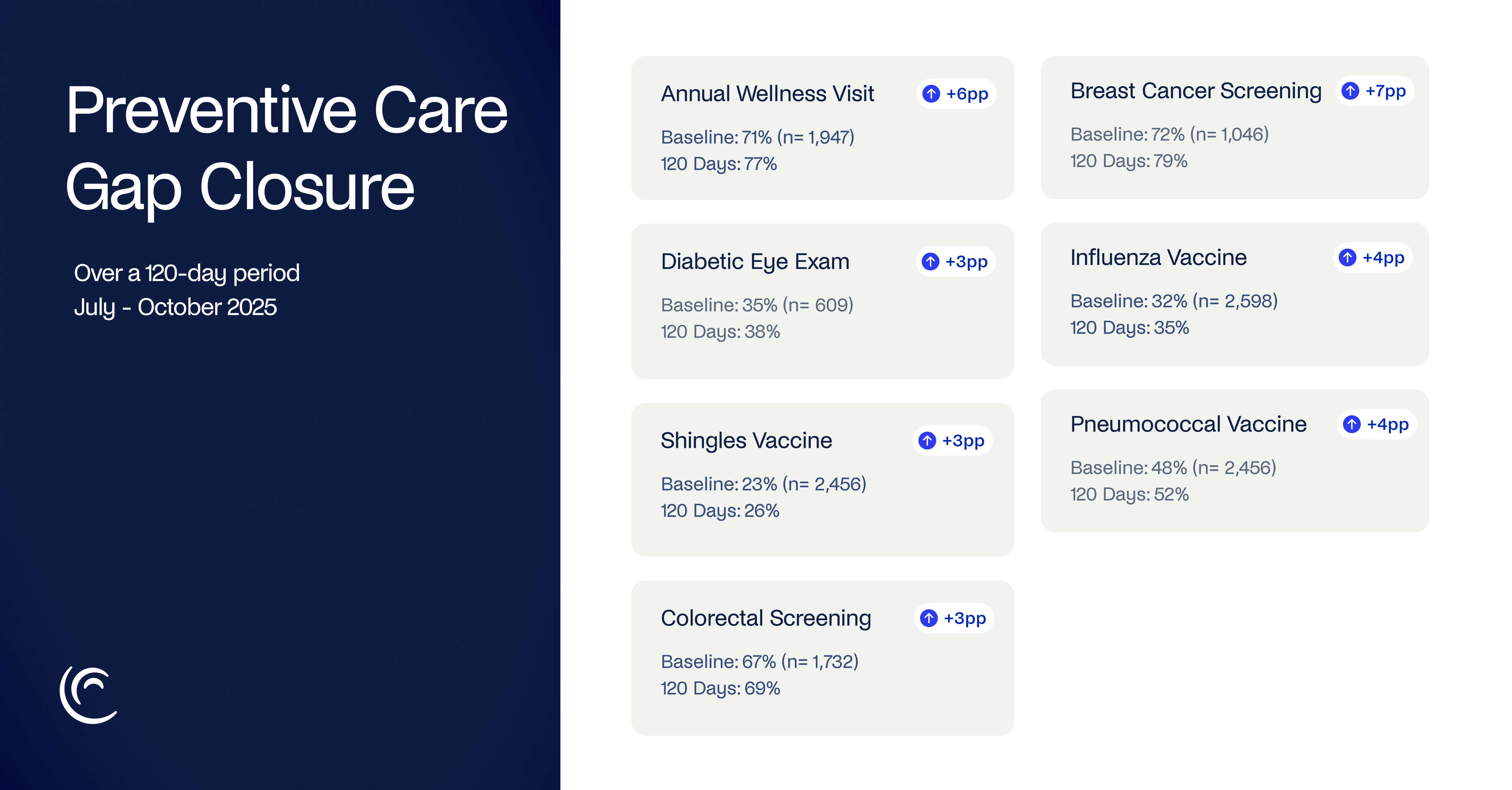
These improvements were achieved through structured, proactive outreach and follow-up, operationalizing care that typically falls between visits.
Addressing social barriers to care
Clinical care alone is often not enough to close gaps. As part of the program, Cadence identified and addressed over 1,300 social needs across the cohort, including:
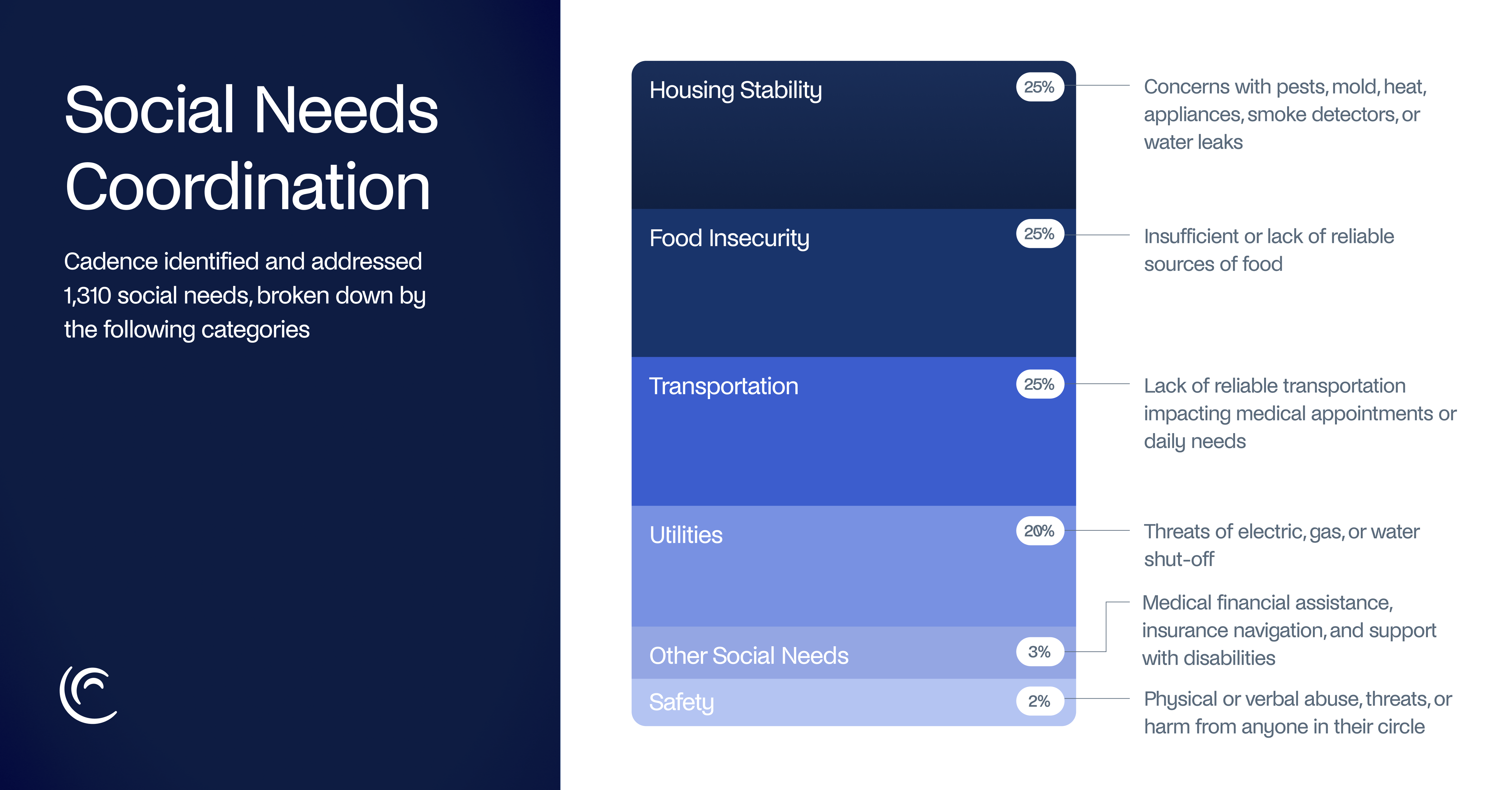
Each of these represents a real barrier to completing recommended care and a key reason gaps persist in traditional models. By coordinating local resources and supporting enrollment in assistance programs, APCM helps remove these barriers and enable follow-through.
Extending primary care capacity
Perhaps most notably, the program demonstrates what it means to extend primary care capacity without increasing provider burden.
In a single month:
- 67% of patients had at least one clinical interaction outside of a visit
- 12,363 clinical encounters were delivered
- Averaging 1.4 touchpoints per engaged patient
This represents a meaningful shift from episodic care to continuous engagement, supporting patients when needs arise, not just when appointments are scheduled.



