Patient with stable cardiac readings; medication adherence confirmed; maintained cardiac rehab and low-sodium diet.
"Felt stable and reassured." 2025 Outcomes Report The Shift to Proactive
The Shift to Proactive
Senior Care
In 2025, Cadence grew beyond remote patient monitoring and became the leader in proactive intervention at scale. Today, we help more than 74,000 seniors manage chronic conditions, stay connected to their care teams, and recover safely at home. As the Medicare population grows faster than ever, health systems are under increasing pressure.
This year, Cadence helped health systems turn the time between visits into opportunities for improvement. Powered by AI and guided by a world-class clinical care team, we delivered better outcomes while reducing burden for clinicians, patients, and health systems. Explore how Cadence is setting a new standard for senior care in our 2025 Outcomes Report.
Cadence Impact Calculator


Clinician capacity
An extension of your practice
Cadence extends the reach of every practice by managing alerts, titrations, and after-hours needs. Our behind-the-scenes, always-on support keeps patients connected and keeps clinicians confident that care is happening exactly as intended.

84,553 Clinician hours saved annually1
3,200 Primary care providers and cardiologists using Cadence nationwide
2.7 hrs Saved per patient, per clinician1
99.5% Of alerts resolved without physician involvement2
24,000+ Medication titrations completed on behalf of primary care providers1
Impact calculator
Your capacity multiplier
84,553
Clinician hours saved annually
24,000
Medication titrations
16,267
Virtual visits completed
48,800
Patient calls & messages handled
99.5%
Alerts resolved without provider involvement

Patient engagement
The momentum behind meaningful growth
Cadence's expansion in 2025 signals staying power. As enrollment grows, so does engagement: patients are consistently active, responsive, and confident managing their health from home, turning daily monitoring into healthier, longer, and more independent living.
74,000 Patients cared for today
23.3M Vitals transmitted in 2025 (up from 8.8M in 2024)3
27,000+ Patients self-activating devices from home3
25 Days per month average frequency of patients taking vitals3
87% Of patients show up to virtual check-ins3
62% Of patients have at least 12 months engaged in program3
9 in 10 Patients repeat readings within 24 hours3
Partner momentum
21 health system partners across 33 states
Across the country, Cadence has become the standard for high-quality remote care. Our partners are proving what's possible when proactive care is scaled responsibly and enables broad patient access.
63% of patients live in rural or underserved communities3
Mission wins
Examples of Cadence's day-to-day impact on patients and practices
Patient with elevated blood pressure; Cadence Care Team arranged medication refill, discussed propranolol increase, escalated to provider.
Caregiver "felt reassured and supported."Patient progressed toward walking goals; BP improved into 120s range with medication adjustment.
"I'm just really happy that it's low."Hypertension patient; RPM monitoring motivated daily checks; maintained ~10,000 daily steps.
Appreciated flu shot guidance while ill.Patient with stable BP/weight, improved oxygen use mobility; caregiver support around the clock.
"Very happy with around-the-clock nursing support."Lifestyle coaching patient; lost 3-4 pounds; exercised 3-4x weekly; Cadence identified medication lapse which resolved.
"Expressed appreciation and scheduled follow-up."Clinical outcomes
A paradigm shift in chronic disease management
Peer-reviewed research demonstrating measurable improvements in cost, utilization, blood pressure control, and guideline-directed therapy.
Peer reviewed & data driven
The Impact of a Remote Patient Care Program on Healthcare Costs and Utilization Among Medicare Patients With Chronic Disease
Published in Mayo Clinic Proceedings, Dec 2025
- $1,428
- Decrease in inpatient spend per patient per year
- 27%
- Reduction in hospital admissions
- 8.4
- Day reduction in length of hospital stay for stroke patients
Scaling Remote Patient Care: The Mechanics of a Paradigm Shift in Chronic Disease Management
Published in NEJM Catalyst, October 2025
- 4.9/5
- Patient satisfaction with an NPS of +40
- 43%
- Increase in blood pressure control
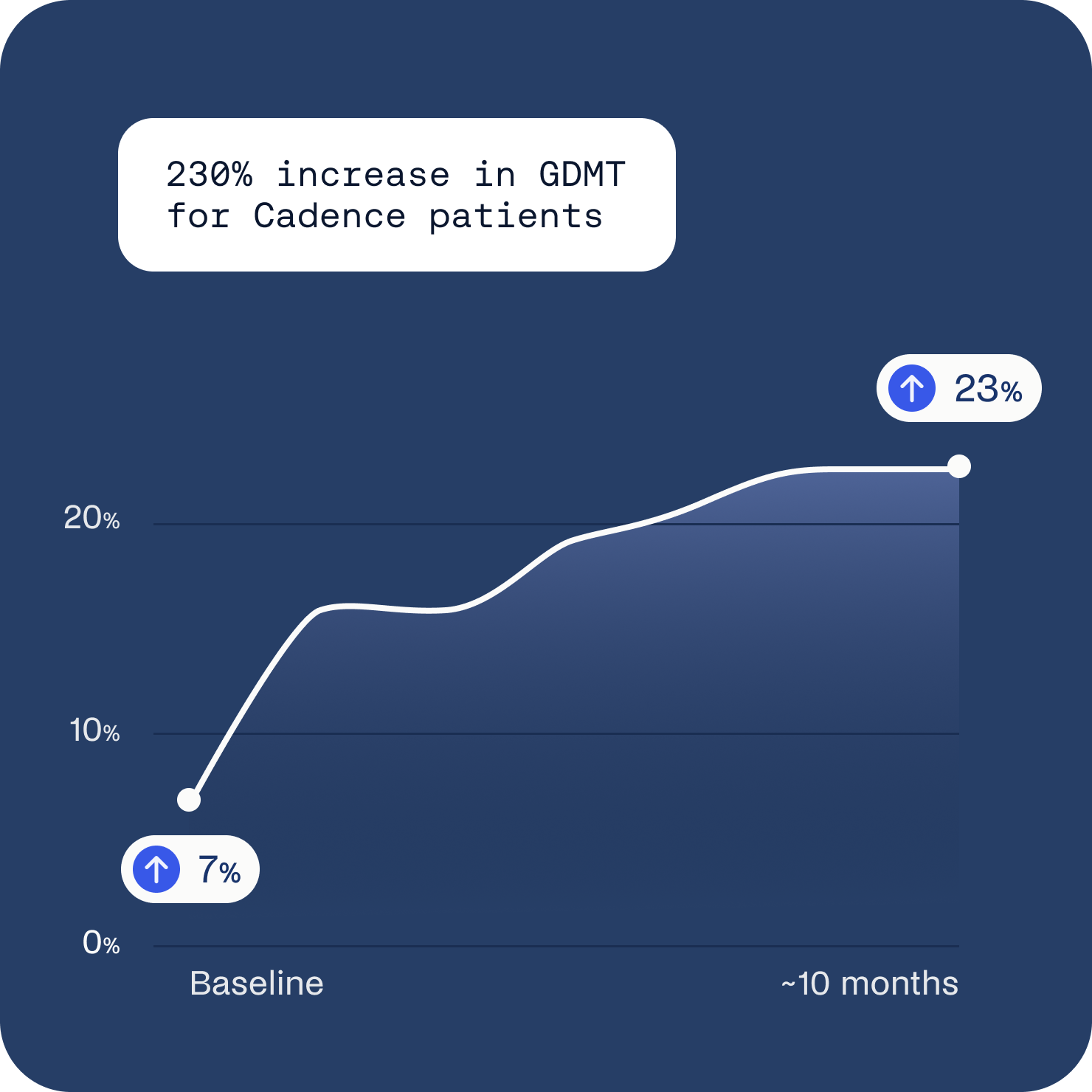
- 107%
- Increase in HFrEF patients on all four pillars of GDMT
Leveraging Remote Patient Monitoring to Effectively Put the Heart Failure Guidelines to Practice
Published in the Journal of Cardiac Failure, Sept 2024
- $1,077
- Monthly cost savings per heart failure patient
- 19%
- Increase in SGLT2 inhibitor use (26% → 45%)
- 5.3
- Systolic BP improved from 131 → 124
Clinical and Engagement Results of a Nationwide Comprehensive Remote Patient Care Hypertension Program
Published in JACC: Advances, July 2025
- 23,638
- Patients, 57% in rural or underserved areas
- 75%
- Patients measuring vitals at 6 months
- 7/5 mmHg
- Average blood pressure reduction
A Remote Patient Care Heart Failure Program Drives Improved Clinical Outcomes and Reduced Healthcare Cost and Utilization
Presented at AHA Scientific Sessions, Nov 2025
- $183
- Total monthly cost savings per patient
- 3x
- Increase in GDMT for HFrEF patients (n=2,697 patients)
- 55%
- Of cohort reside in rural and underserved areas
Intelligent care
AI that improves clinical outcomes
Cadence's clinical intelligence automates documentation, highlights what needs attention, surfaces key patient signals, nudges timely interventions, streamlines team workflows, and syncs directly with EHR.
Automates documentation
Highlights what needs attention
Surfaces key patient signals
Nudges timely interventions
Streamlines team workflows
Syncs directly with EHR
Introduced 2025
Lifestyle Coaching Copilot
Uses AI to add visit context and sentiment insights, helping care teams personalize communication and deepen trust.
31% Fewer low patient survey scores
20% Fewer early disenrollments
35% Fewer disengaged patients within 30 days
22 min Per care plan generation (13 min saved with Copilot)8
Testimonials
The impact, first hand
"When a clinician goes to Cadence, they can actually go into Epic, see every one of their patients who are not meeting goals, and make a very simple workflow. Then you have a group of APPs who are going to follow your approved pathways for making sure those patients get under control. That would've been something I would've only dreamed about in residency."
Dr. Jessica Schlicher Chief Medical Officer of Virtual Care and Digital Health, Providence
"When we deployed, we started with pilot practices and positioned Cadence as an extension of us -- the value for our physicians, the why of monitoring and intervening in a patient's care between visits. We're now doing true panel management rather than just individual patient management, and it's changing the entire aspect of care."
Dr. Anuj Mehta Chief Clinical Officer, Hackensack Meridian Health
"I learned about the program following my stroke. My doctor, Dr. Cobo, told me that I had been referred to the program. This is the first time I've ever seen the difference that how I take care of myself directly translates into my wellbeing."
Lynda Loy Wilgus Patient, Chicago, Illinois
"I always had high blood pressure and I chose not to medicate myself for it, which was a mistake. [With Cadence] I've learned to eat with portion. I've lost 40 pounds recently. That's helped in reducing my blood pressure. Now, my BP was 107 over sixty eight."
Alan Katz Patient, Chicago, IL
Program launches
Two new models of proactive care
Advanced Primary Care Management (24/7)
Primary care is stretched thin. APCM identifies early care needs and supports patients between visits, closing overdue clinical and social care gaps.
2.44 Care gaps per patient identified and closure initiated by Cadence9
22% Improvement in closure rate through APCM support9
American Heart Association Connected Care™ (Post-Acute Care)
Nearly 1 in 4 heart failure patients are readmitted within 30 days. American Heart Association Connected Care™, Powered by Cadence, extends evidence-based support into patients' homes immediately after discharge, reducing preventable readmissions.
88% Of patients activate devices and report vitals within 14 days of discharge11
3 Health systems partnered: Montage, Lifepoint Health & Texas Health Resources
24/7 care
An industry-leading clinical Care Team
Cadence's multidisciplinary team of medical directors, nurse practitioners, registered nurses, and medical assistants provide consistent, personalized care for patients 24 hours a day, 7 days a week.
22,800 Interactive minutes spent with patients every day12
244K Remote visits with patients led by Cadence's Care Team annually3
3.1M Minutes of interaction with patients annually3
Policy leadership
Leading the charge for high-value remote patient care
In 2025, Cadence co-founded the Remote Monitoring Leadership Council -- a coalition of digital health leaders working to raise the bar for high-quality, technology-enabled care.
Recognition
Nationally recognized for innovation and impact




Setting a new standard
In 2025, Cadence proved what's possible when technology and clinical expertise align: outcomes improve, costs are reduced, and patients feel more connected and supported than ever. This year showed that this proactive care model is a working, scalable system delivering real results for seniors and the health systems that serve them. Together with our partners, we're setting a new standard for modern senior care.

A win for patients, clinicians, health systems, and payers
Capacity, outcomes, and revenue without added risk.